

Are COVID-19 vaccines the only effective treatment and prevention option for SARS-CoV-2?
In part 2 of the 5 in the vaccine mandate pillars series, I examine alternative methods for prevention, transmission, and reduction of death and hospitalization contrasted to current US vaccines.

Introduction
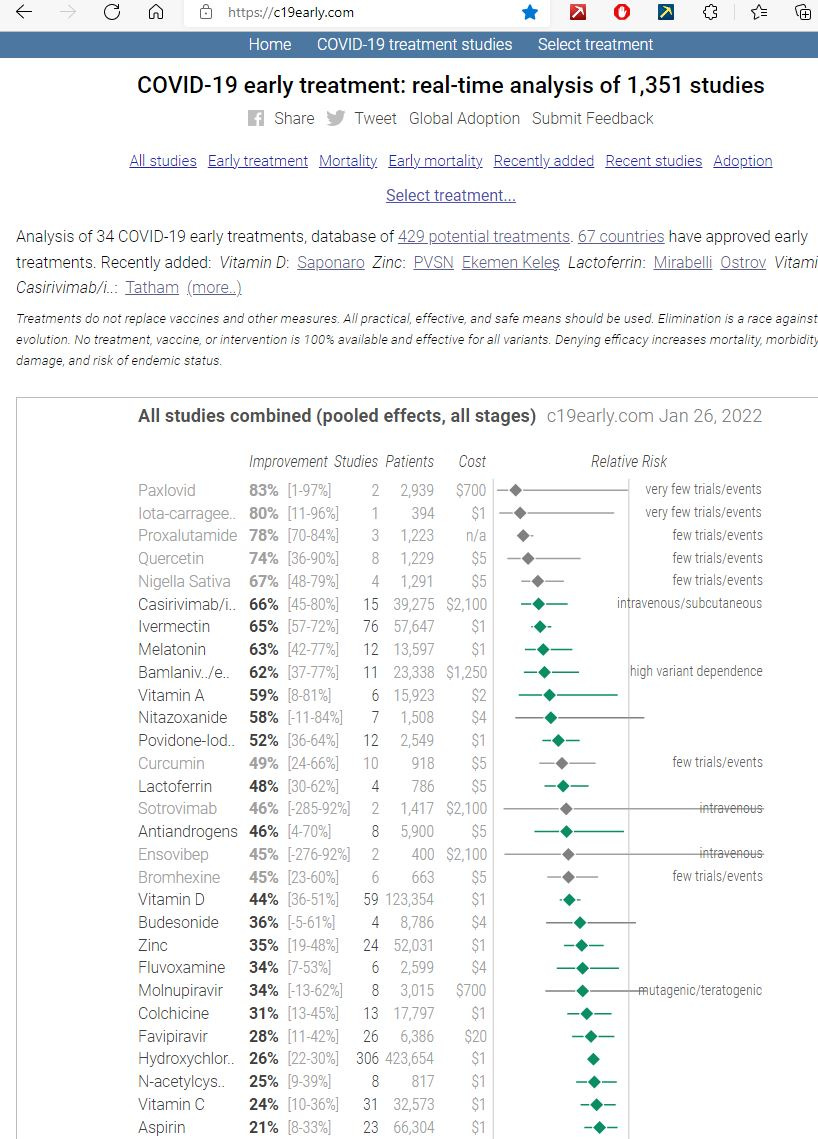
The above graphic is from COVID-19 early treatment: real-time analysis of 1,351 studies - the best source I can find for COVID-19 therapeutic data, studies list, and analysis that is continually kept updated. I refer to this site (https://c19early.com) quite a bit in this article since the issue brought up for the first pillar of vaccination mandate justification is exclusivity - the assumption that no alternative treatments can work.
Currently, no alternative therapies other than monoclonal antibodies (which are now being restricted by the Biden administration) have been endorsed by the CDC, FDA or NIH, at least not in mainstream media channels. Although the FDA approved monoclonal antibody treatments for use by hospitals not only for treatment but for prevention - FDA authorizes REGEN-COV monoclonal antibody therapy for post-exposure prophylaxis (prevention) for COVID-19 | FDA, few Americans are aware of this as there has been virtually zero mention of this by Dr. Fauci, Dr. Walensky or most media outlets.
UPDATE - 1/25/2021: The FDA now has halted the emergency use authorization (EUA) of two monoclonal antibody treatments on the justification that they are not effective for Omicron - https://www.msn.com/en-us/health/medical/reckless-monoclonal-antibody-treatment-sites-close-following-fda-decision-to-remove-emergency-use/ar-AAT6LL8. Never mind that they were very effective for the Delta variant which is still circulating - I wonder if they will also remove the approvals for the vaccines since they also don’t work against Omicron based on studies cited later on in this post).
Emerging therapies including ivermectin or any off-label use of drugs such as fluvoxamine and Hydroxychloroquine are prohibited with censure an inevitable consequence of those who promote them. In addition, information concerning other prophylactic measures such as vitamin D supplementation or lifestyle behaviors such as weight control has rarely been shared by any of the public health authorities.
In this article, I review the safety and effectiveness of alternative options to COVID-19 vaccination to determine if they may be viable alternatives for certain risk groups. The purpose of this post is not to provide a definitive answer, but to share research in this area that will be integrated with vaccine safety data to determine if some of these alternatives are preferable to vaccination. I organize these alternatives in the following three categories:
Lifestyle behaviors that may reduce risk of infection or severity upon infection including weight control, vitamins, supplements, and exercise
Therapeutics including off-label drugs and monoclonal antibodies that may reduce risk of infection or severity upon infection
Natural immunity
Lifestyle behaviors
Since the start of the pandemic, including prior to vaccine rollout, the only behaviors advocated by US national health authorities have been lockdowns with wearing of masks and social distancing. In the beginning there was discussion of surface sanitization but that has been relegated to being of lower value even by the CDC (You Can Lighten Up on Sanitizing Surfaces for COVID-19 (healthline.com)). More detail regarding surface safety including food safety is at Food Safety and the Coronavirus Disease 2019 (COVID-19) | FDA. These lockdown protocols have been implemented mainly via policy including mandates.
Lockdowns
Lockdowns have shown no statistically significant correlation for reducing COVID-19 cases, hospitalizations, and deaths over the long-term. Factoring in the adverse health effects, it has had a negative impact. The damage of the lockdowns has been evident since May, 2020 but largely ignored - Lockdown Suicide Data Reveal Predictable Tragedy – AIER. Despite the emergence of the vaccine and close to the same number of COVID-19 deaths in 2021, excess deaths are significantly higher in the US and much of the world than 2020. Much of the death is due to delayed medical procedures including cancer screenings, increased suicides, increased drug overdoses, and effects of increasing obesity in the population. The Substack article Lockdowns - A Post from July, 2021 - by JB (substack.com) provides an extensive analysis with references to many studies from peer-reviewed journals.
Masks
Likewise, mask wearing has been extensively promoted with mandates nationally, locally, and corporately, but statistically significant effectiveness has not been established through any large random-controlled-trial (RCT) and the side effects of masking may promote more harm than health. This is still true to a lesser degree with the use of higher quality N-95 masks. An extensive review of mask studies is here: More than 150 Comparative Studies and Articles on Mask Ineffectiveness and Harms ⋆ Brownstone Institute
Social Distancing
Social distancing for short interactions provides some benefit, but it is not practical for many working situations since the SARS-CoV-19 aerosol particles remain airborne far longer than individuals remain stationary, even if that is only a few minutes. The majority of transmission occurs among close contacts, whether they use masks/social distancing or not (https://www.toronto.ca/wp-content/uploads/2020/10/8de9-COVID19-Transmission-Aerosols-Ventilation.pdf )
Given that prevention of SARS-CoV-2 is limited using lockdowns, masking and even to a certain extent social distancing, we now consider studies of other alternatives not frequently mentioned by mainstream media sources or public health authorities for effectiveness:
Weight control including obesity
Vitamin D and other vitamin/mineral supplementation
Exercise
Weight Control
Public health authorities rarely mention the impact of obesity on general health, let alone COVID-19. Yet, obesity is the highest comorbidity factor for death from COVID-19. Simply maintaining a correct weight reduces hospitalization from COVID-19 by around two times based on a CDC study showing that the incidence of obesity for those with COVID-19 is 78% versus 42% for the general population - Body Mass Index and Risk for COVID-19–Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death — United States, March–December 2020 | MMWR (cdc.gov). Obesity has greatly increased since the pandemic, largely due to the effect of lockdowns, which is another reason that lockdowns may have actually had a negative overall impact on reducing COVID-19 hospitalization and death - Pandemic may have pushed millions more into obesity in 'perfect storm' (telegraph.co.uk)
Vitamin D and other vitamin/mineral supplementation
Multiple studies have shown a correlation of low vitamin-D levels and elevated cases, hospitalizations, and deaths from COVID-19. Some studies have erroneously concluded that vitamin D supplementation is not effective based on providing Vitamin D supplements in late stage COVID-19. This is misinformation in that it takes 6 to 8 weeks for Vitamin D supplementation to take effect based on studies on treatment protocols - Vitamin D Deficiency - StatPearls - NCBI Bookshelf (nih.gov).
Other vitamins and supplements are also associated with reducing risk of death from COVID-19. These benefits are compounded by ensuring adequate levels of all vitamins and minerals since absorption of some vitamins and minerals are negatively affected by inadequate levels of facilitating vitamins or minerals. Below is a list of some tudies outlining the benefits of Vitamin D for reducing risk of COVID-19 cases, hospitalizations, and deaths
Vitamin D and COVID-19: An Overview of Recent Evidence (nih.gov)
Vitamin D Deficiency and Covid-19: - by Heather Heying (substack.com)
Vitamin D for COVID-19: real-time analysis of all 210 studies (c19vitamind.com)
Exploring links between vitamin D deficiency and COVID-19 - PubMed (nih.gov)
One of the best sources for Vitamin D is sunshine. This also is an adverse outcome from policy makers who advised individuals to stay inside. Vitamin C, Zinc, Magnesium, and Vitamin K are also associated with a stronger immune system based on this analysis - Supplements to Boost Your Immune System to Prevent or Fight Off Covid-19 (substack.com). Meta-analysis of individual use of Zinc, Vitamin C, and Vitamin D are listed here:
Vitamin D for COVID-19: real-time analysis of all 210 studies (c19vitamind.com)
Zinc for COVID-19: real-time analysis of all 55 studies (c19zinc.com)
Vitamin C for COVID-19: real-time analysis of all 48 studies (c19vitaminc.com)
Ensuring adequate levels of all these vitamins provide a compound effect to ensure stronger immunity - Nutritional risk of vitamin D, vitamin C, zinc, and selenium deficiency on risk and clinical outcomes of COVID-19: A narrative review - PubMed (nih.gov)
Exercise
The impact of exercise as a preventative and survival measure for disease including COVID-19 has also been absent from the public health discussion. The opposite has been true in that lockdowns have been pursued that shut down access to gyms causing not only obesity but also reduces muscle tone and increases the amount of body fat regardless of weight status:
Obesity – already known as a significant contributor of hospitalization and death from COVID-19
Body fat – related to obesity – but this study shows that higher body fat is associated with poorer outcomes from COVID-19. Therefore not only health weight, but muscle tone may reduce likelihood of severe outcomes - Does abdominal fat affect COVID-19 outcomes? (news-medical.net)
Therapeutics
Throughout the pandemic the FDA as well as the WHO and most countries have taken aggressive measures to prevent the use of any off-label treatments even for prophylaxis or early treatment when the risk of adverse events from those drugs with extensive safety records (far better safety than the COVID-19 vaccines based on data from the CDC Vaccine Adverse Event Reporting System – Open VAERS system for querying CDC VAERS data.
Except for the new anti-COVID-19 drugs being developed by Pfizer and Merck, the NIH has not facilitated any significant research in the use of therapeutics. However, studies large enough to be of statistical significance have been done, including many RCT studies. The site COVID-19 early treatment: real-time analysis of 1,337 studies (c19early.com) maintains a continuous meta-analysis of studies and outcomes for the major early treatment protocols, including not only off-label drug use for COVID-19 such as Ivermectin, but also supplements. In addition to this, the reader is directed to correlative analysis of usage of Ivermectin that has been established in multiple countries. These studies are listed below:
Uttar Pradesh, India:
Of course a “fact check” was published shortly after that disputing this, but Ivermectin Denial Tough With This Information | peckford42 (wordpress.com) addresses this.
Africa correlation to lower COVID-19 case:
Ivermectin, Hydroxychloroquine, and Fluvoxamine are well-established statistically as successful for prevention and not just treatment due to the sheer quantity of positive RCTs. That these drugs are not being promoted and actually being banned by the FDA does not take away from that. In the final article of this series, we will address the issue of censorship and what motivations may be behind the obvious suppression of important scientific peer-reviewed scientific research on COVID-19 vaccine alternatives. Meta-analysis of studies of four common drugs proven to be effective in off-label use with no significant safety (we will examine the detailed safety data of these versus the vaccines in the next post in the series) issues include:
Ivermectin for COVID-19: real-time analysis of all 144 studies (c19ivermectin.com)
HCQ for COVID-19: real-time analysis of all 374 studies (c19hcq.com)
Fluvoxamine for COVID-19: real-time analysis of all 12 studies (c19fluvoxamine.com)
Quercetin for COVID-19: real-time analysis of all 15 studies (c19quercetin.com)
Monoclonal antibodies have proven successful against the Delta even if not as much against the Omicron which has much lower hospitalization and death figures. Monoclonal antibodies is an adaptive technology and trials for not only treatment but for prophylaxis continue to be conducted with modifications to the antibodies to keep pace with the variants. Omicron does not signal the end of monoclonal antibodies for both prevention and treatment of COVID-19 - Anti-SARS-CoV-2 Monoclonal Antibodies | COVID-19 Treatment Guidelines (nih.gov). Meta-analysis of some of the monoclonal antibody treatments are listed here:
Sotrovimab for COVID-19: real-time analysis of all 7 studies (c19sv.com)
Casirivimab/imdevimab for COVID-19: real-time analysis of all 23 studies (c19regn.com) (AKA Regeneron)
Bamlanivimab for COVID-19: real-time analysis of all 18 studies (c19ly.com)
The only question is how effective the therapeutics are compared to the vaccine but given the reduced efficacy of the vaccine against ever-evolving variants, the assertation that mass vaccination of all demographics is required is called into question. There are some drugs that are being used at the hospitalization stage of COVID-19 directed by the FDA, but their efficacy and safety appear worse compared to many of those banned by the FDA - Remdesivir for COVID-19: real-time analysis of all 37 studies (c19rmd.com, Remdesivir and Acute Renal Failure: A Potential Safety Signal From Disproportionality Analysis of the WHO Safety Database - PubMed (nih.gov))
When determining exclusivity of the vaccine for every demographic versus strategic use of therapeutics, both safety and efficacy must be analyzed across all age groups. The Omicron variant introduces new dynamics in that monoclonal antibodies are not nearly as effective and there is not much data on effectiveness of therapeutics for this variant yet. However, the vaccine has also proven ineffective against Omicron without boosting which introduces additional safety concerns. The Omicron variant is also much milder than the Delta or original variant, so this brings up another issue as to the urgency for global vaccination. The topic of exclusivity will be revisited in the remaining articles in the series with a conclusion in the final post in the series.
Natural Immunity
No exception for natural immunity (wherein a person was previously infected by COVID-19) from has been afforded by the mandates. In many jurisdictions worldwide, this is done, but not in the United States. Below outline some of the policy exceptions worldwide for natural immunity:
Germany Treats Natural Immunity the Same as Vaccination | National Review
15 countries recognise Hungarian immunity certificates! – Daily News Hungary
146 Research Studies Affirm Naturally Acquired Immunity to Covid-19: Documented, Linked, and Quoted ⋆ Brownstone Institute outlines 146 studies, many peer-reviewed outlining the benefits of natural immunity. Many of the studies indicating multiple-fold better and longer-term protection against COVID-19 than the vaccine. This should not be surprising since the purpose of a vaccination is to provoke a human immune response as the vaccine is not the actual response. It is only logical that an innate human response against the actual virus instead of a simulated virus should be better. The justification for vaccination has traditionally been to avoid getting a dangerous illness. However vaccination against an already-acquired disease has never been a component of mandatory vaccination - Comparing Natural and Vaccine Immunity (michigan.gov).
Although natural immunity is proving not very effective against Omicron, the vaccine is also not showing to provide much benefit except with boosting (Finally: CDC Admits Natural Immunity Acquired Via Previous Infection Better Than COVID Vaccines : US : Christianity Daily. In fact, data from the UK is now showing negative efficacy of the mRNA vaccines against Omicron without a booster - With Omicron: Negative Efficacy Like Never Before (substack.com). This may be due to the effect that Dr. Paul Alexander refers to here whereby “programmed” immunity associated to the spike-protein only may actually be suppressing a superior natural immune response - OMICRON resistance to vaccinal antibodies (Abs) is PERFECT; vaccinal Abs will no longer 'outcompete' the INNATE antibodies (in children/young persons) thus INNATE are 'set free' to STERILIZE the virus (substack.com)
Boosters introduces additional safety risks which will be discussed in the next post in this series.
Coming Next
In the next post in this series, I examine the safety issues of the vaccine and compare to alternatives for prevention and treatment of COVID-19. Also, the compounding of alternate options together (lifestyle behaviors, therapeutics, and natural immunity) must be evaluated in their overall impact to determine if mandatory global vaccination is justified by the risk/benefit. This along with examining the risk of COVID-19 is an important aspect for determining the exclusivity of the vaccine-only approach.
Excellent!